



Guest blog: Hubris Syndrome – Metrics and Meaning. (2015)

Reflecting on the Hubris in Business and Management symposium hosted by Eugene Sadler-Smith and the Surrey Business School at the University of Surrey on 20 May 2015, the author Marc Atherton asks “what form of measure could be appropriate for assessing Hubris Syndrome?”
Daedalus: Hubris Syndrome – Metrics and Meaning.
Marc Atherton MSc, CPsychol, CSci, AFBPsS, FRSA, MRAeS, EuroPsy
“Strive not to be a success, but rather to be of value.” Albert Einstein
Much has been written recently around the concept of hubris in politics and business driven by the recognition that the (mis)behaviour of specific individuals has been instrumental in recent well known collapses of complex organisations with significant collateral damage to people’s lives and finances. There is a wide recognition that in many cases these collapses are the result of a particular form of self-belief and behaviour which Owen et al (1) have termed Hubris Syndrome (HS).
A symposium (Hubris in Business and Management) was hosted by Surrey Business School at the University of Surrey on 20th May 2015 to bring together researchers and practitioners for an exchange of ideas in current state-of-the-art in hubris research. The symposium was hosted by Eugene Sadler-Smith. It is a consideration of the symposium that has led to this note being written. This article highlights some key issues and constraints in taking the concept of HS out of the research space and into the practice space for discussion.
Owen et al (2) describe HS as a constellation of 14 characteristics which shares a common core of characteristics with Narcissistic Personality Disorder (NPD) as defined in the Diagnostic Systems Manual (3). Hubris Syndrome is a more complex pattern than NPD and for it to be categorised it is assumed that at least 5 of the 14 defining characteristic be present (4).
It is this point that forms the basis for this article. In defining HS as being present we are presuming a model which is common in both Clinical and Occupational Psychology – that there is an underlying psychological construct (HS) that will manifest itself in behaviour which can be defined and measured in some way subject to certain psychological and statistical principles.
Owen et al suggest that at least five characteristics be present to facilitate a ‘diagnosis’ of HS. A framing question put forward in this article is what form the diagnosis could take, what would be considered for it be valid and what could be done with the diagnosis?
Before touching on this it is worth considering the terms used. Hubris has a modern common usage to mean over-weaning pride and self-belief in one’s own capabilities and infallibility. In Classical Hellenic culture it also had an aspect of being dismissive of the opinion of others and disrespecting them as people (5). In Hellenic culture it went hand-in-hand with a number of other concepts that are worth incorporating in the discussion; Nemesis, Perigyros and Panegyrics.
Nemesis (6) is the downfall of the individual prompted by the Gods for exhibiting hubris and not being sufficiently humble. It usually took the form of a fall from grace and subsequent ruin (cf. Icarus in a metaphorical and literal sense).
Perigyros is a concept which in modern Greek translates as ‘surroundings’. In the Hellenic period it included the concepts of both physical and social surroundings – environment and social circle might be a good interpretation. It is from the perigyros that panegyrics arise.
Panegyrics (7) have evolved to mean unconditional and excessive praise heaped upon a leader or person with power which can cause them to believe in their own omnipotence and omniscience. The original concept was Hellenistic but the tradition continued and was well established in the Roman period.
The Republic of Rome is perhaps also a source of insight into the role of panegyrics as a risk factor for hubris and a response to it.
Victorious generals returning to Rome were required to leave their legions at the River Rubicon to the north of the city. A General who did not do this was in breach of the Laws of Rome and the authority of the Senate and would be declared an enemy of Rome (hence the English expression ‘crossing the rubicon’ for a decision from which there is no going back).
The victorious general that complied with leaving his legions on the northern side of the Rubicon was heralded a hero and given a victory parade through Rome. At his side during the victory parade would be a slave whispering in his ear ‘memento mori’ (~ ‘remember your mortality’) to remind him that no man was greater than the People and Senate of Rome and that glory was fleeting. This might be seen as a form of ‘anti-panegyric’ social mechanism designed to limit the possibility that a Roman general might succumb to hubrisistic tendencies and decide that the Republic and the Senate needed a little ‘guidance’.
One moral of this story was summed up by John Donne;
“No man is an island, entire of itself; every man is a piece of the continent, a part of the main.”
This observation also considers that, as recent findings in Social Psychology and Behavioural Economics have shown, individuals are subject to circumstances and situational influences to a much greater extent than we would like to believe.
Dr Arlo Brady of the Freud Brewery Centre, in an article in the Huffington Post (9), identified an issue with modern corporate leaders living their lives in the splendid isolation of the luxuriously carpeted C-suite offices with no contact or comprehension of the world of ‘Joe the plumber’. Add in gated communities, limousines and private jets and the isolation becomes almost total. It is reasonable to wonder if this isolation and pampering might not be a risk factor in the development of hubris. Where is the slave whispering in the ear of the corporate, political or bureaucratic potentate?
Given the above discussion the issue then becomes one of what form of assessment and response to HS for individuals in organisational settings might be viable. If HS is to be defined as an extant characteristic then it must be possible to consider what form a diagnostic approach might take. From Thurstone, Thorndike and Rasch (8) we have the principle that it is possible in the social sciences to construct valid measures of psychological and social constructs that have rigour, reliability, scalability and validity. This foundation allows us to ask a basic question;
“what form of measure could be appropriate for assessing HS?”
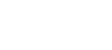
The approach suggested in this article is to use a potential solution space which has two primary axes and bounds the space within which any HS diagnosis could lie;
1. Idiographic versus Normative
2. Prescriptive versus Descriptive.
A minimum consequence of the Owen et al approach in highlighting the similarity of HS to the DSM 4 definition of NPD as a state which has categorical symptoms and a clinical mitigation approach is whether an analogous diagnostic and treatment model is applicable to HS. The DSM approach is firmly in the Prescriptive half of the model in this conception.
The question arises then as to whether the approach to HS should, or indeed can, follow a similar model. A clarification of the principles underlying the DSM model is worth making.
The DSM model is one which assumes a clinical diagnosis backed up by the power of authoritative documented definitions, professional accreditation, legal sanction and the ability of the courts to subordinate the rights of the individual under certain specific conditions. The basic position of the DSM approach is to place the assessment and subsequent actions in the Prescriptive part of the solution space above – either in the normative or idiographic quadrant depending on the construct being considered (for example psychotic, schizophrenic or depressive states). States being assessed in these quadrants are typically seen to be outside the range of ‘normal’ variation and are seen to pose a significant and real threat to the individual and/or others.
Assessments in the Descriptive sector tend to be less powerful and have a lesser force of sanction associated with them where present. Personality Type Inventories might fall into these quadrants – the assessment is dealing primarily with states within the ‘normal’ range of variation where the consequences of the variation are considered to be acceptable.
When considering the possible position in this notional space where an assessment and response regime to HS may lie we are constrained with recognizing that we are probably operating outside of the currently accepted legitimacy of the DSM approach which may initially leads us by default to the descriptive sector.
Outside of the clinical setting, in the business world, we are faced with a number of key considerations that directly affect the form of assessment and ‘response’ that might apply. If HS is not classified as a distinct form of Mental Illness, then it becomes challenging to move forward for a number of reasons;
1. A HS assessment would be dealing with an incipient condition that may, under certain circumstances, actually be beneficial in the short term. Assessing incipient conditions, in effect attempting to predict that someone may develop HS and that it may result in damage or loss to others, is a difficult legal hurdle to overcome as our judicial system is based on the presumption of innocence until proven guilty.
a) As mentioned this can only be circumvented when the potential psychological state, the assessment and the likely consequences are sufficiently weighty to warrant preventative action by the authority of the State (eg. sectioning an individual for their own or others safety in the UK).
2. A HS diagnosis may be difficult to implement due to political constraints. Where the power to command lies in an individual then issues of how the diagnosis is made and how its legitimacy is maintained poses a challenge. An imputation of HS may well result in a political response that is difficult to overcome in a non-court setting. One can think of the difficulty faced in removing several notable high-profile political and business figures from both sides of the Atlantic over the last 25 years.
3. Issues around the Reliability and Validity of any psychological assessment for HS are bound to be relevant to any solution. Given that we might be dealing with an incipient condition, with some uncertainty over which sub-set of the 14 core traits (Owen et al) are pertinent and present then the issues of assessment Reliability and Validity become relevant. With a likely small sample size, any normative statistical analysis would have limited power and generalisability. Given this it may be an issue around predictive power and validity and any assessment could face significant legal challenges.
4. Given the above, if it is decided that an assessment for HS is appropriate we are faced with the question of its format. Is to be akin to;
a) A clinical interview in which case who is accredited to perform the interview and to whom does that individual owe a primary duty of care?
b) A neuro-psychological assessment which requires that a definition of a pragmatic content and process be outlined.
c) A self-report approach in which case how is it to be created, validated, administered, scored and feedback provided to the relevant stakeholders?
d) A ‘360’ approach in which case how are raters to be selected and how are views to be aggregated and feedback managed?
e) An approach based on the use of modern social media data analytics and expert opinion to look for patterns of indicator precursors which might lead to HS (in which case how is the model constructed, calibrated and executed)?
f) An approach based on the use of linguistic analysis in which case what model of indicator language is used and how are relevant texts selected for inclusion given the prevalence of corporate communications and PR speechwriters?
g) A combination of some or all of the above?
These issues are, I believe, pertinent to the possible space in which a solution lies. For example within the Financial Services sector in the UK, the Financial Conduct Authority has requirements that individuals need to meet to be a Registered Person with legal accreditation to be employed in a regulated organisation. As a thought experiment one could wonder how HS could be introduced into this regime in a practical way and use the outcome of this as a guide to action.
Another avenue that could be worth exploring lies in the professional organisations which represent businesses and their staff – in the UK context these could include the Boards of Directors, Unions, the CBI and the IOD as well as the sector Regulators. An assessment of what might be acceptable and feasible from their perspectives could help to put a boundary around the areas in which a practical solution to HS might lie.
Assuming that we can develop an acceptable, reliable, valid and practical assessment approach for HS (which I believe we can subject to not knowing how acceptable, reliable, valid and practical without appropriate research) it leads us to the issue of what consequential actions are taken post-assessment?
1. Does the assessment have a continuum of severity which leads to a range of outcomes from a (mandatory?) coaching intervention at the moderate end to redundancy and disbarment at the severe end?
2. Is it possible to have counseling and then have the assessment redone to demonstrate that an individual no longer shows an incipient HS diagnosis and as such could seek to be reinstated?
3. To what extent is the problem seen as residing in the individual versus the individual-environment interaction and how might this affect the rights of the individual and the duty of care liability of the organisation (consideration could be given to the HSE approach to Stress Management where at the Primary Level the obligation is on the organisation to mitigate the conditions leading to stress (10))?
I am reminded of a movie – The Godfather – at this point. In this movie the character played by Robert Duval is the consigliere to Al Pacino’s ‘Don Corleone’ – his duty is to speak truth to power to keep it grounded. Eventually Don Corleone moves the consigliere aside when his advice is no longer appreciated in changing circumstances. Is this a risk we face with a solution to mitigating HS in the workplace using a non-blame, preventative approach and a duty of care to notify relevant stakeholders in a way similar to a Psychologist’s duty of care?. If so would this lead to an automatic external sanction response or an internal dialogue?
There are clearly many issues to be considered and this piece is intended to stimulate debate and stakeholder identification and engagement to further the development of the concept of HS definition and assessment in the workplace. Perhaps it would be simpler to have HS, and its incipient symptoms, classified as a DSM 5 condition subject to the full legal implications of that decision (the USA has a broad reach in what it considers its legitimate legal and economic sphere of interest) and consider that we have done all we can to deal with the problem. Personally I feel that this would be to abrogate our responsibility to the individual, the organisation and the broader society to find a positive way forward in eliminating the risks posed by HS in our 21st Century economy whilst advancing the cause of leadership in its broadest sense.
1. Owen D and Davidson J (2009) Hubris Syndrome: An acquired personality disorder? A study of US presidents and UK prime ministers over the last 100 years. Brain 132: 1396-1406
2. Hubris in leadership: A peril of unbridled intuition? Guy Claxton, David Owen and Eugene Sadler-Smith, Leadership published online: 12 December 2013
3. DSM 4, APA, 2000 (replaced by: DSM 5, APA, 2013)
4. Hubris Syndrome in leadership is an obstacle to the transformation of organisations. Speech by the RT Hon Lord Owen, Sol Global Forum, Paris. 20 May 2014
5. http://www.britannica.com/topic/hubris (2015)
6. http://www.oxforddictionaries.com/definition/english/nemesis (2015)
7. http://www.britannica.com/art/panegyric (2015)
8. A History of Social Science Measurement, Benjamin D Wright, Educational Measurement Issues and Practices, September 1997
9. http://www.huffingtonpost.co.uk/dr-arlo-brady/the-modern-leader-_b_6782030.html
10. http://www.hse.gov.uk/stress/standards/, (2015).
Marc Atherton MSc, CPsychol, CSci, AFBPsS, FRSA, MRAeS, EuroPsy
44 (0) 77 9613 80v4, marcatherton@allaxa.co
Leave a comment
Back to the top